
Post op imaging in Congenital Heart Diseases
- Dr Ayush Srivastava
- Apr 18
- 6 min read

Extra Cardiac Palliative Surgeries
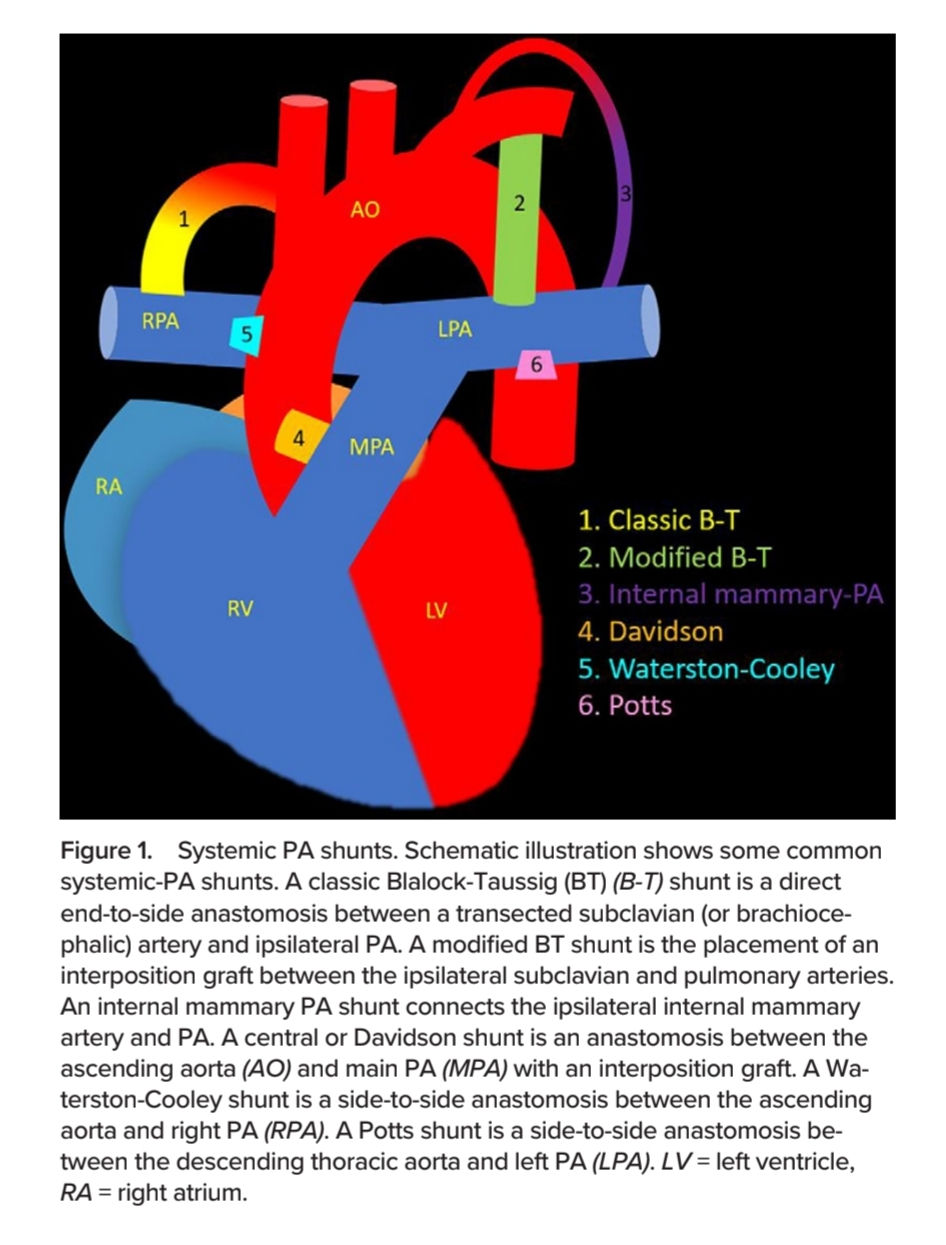
Systemic Arterial → PA Shunts
To oxygenate the cyanotic blood.
Systemic - PA shunts increase the blood flow to the pulmonary arteries in a regulated manner without overcirculation or heart failure.
It leads to enlargement and growth of pulmonary arteries.
These may be a part of stage I palliation in pts with single ventricle morphology (tricuspid atresia, hypoplastic left heart syndrome)
A single ventricle maintains both systemic and pulmonary circulations operating in parallel → gets compromised by chronic volume overload.
Hence single ventricle palliation involves:
Systemic circulation → supplied by the single ventricle, and
Pulmonary circulation → passively via systemic veins through Glenn and Fontan shunts.
Fontan procedure requires normal pulmonary vascular resistance and hence is not feasible in the neonatal period with associated high pulmonary vascular resistance.
In addition, the pulmonary and systemic vessels are small in neonates, with catch-up PA growth required before performing a Fontan procedure.
Pulmonary arterioles can multiply in number until 3 years of age and increase in diameter until 11 years of age.
Glenn shunt and Fontan procedure are performed in subsequent stages to adapt to the evolving physiology of the child.
Systemic-PA shunts also help facilitate the growth of PA in pulmonary atresia.
Types of Systemic-PA Shunts
Blalock Taussig
Potts
Waterson Cooley
Davidson
Sano
Blalock Taussig Shunt
Classic BT: End-to-end Subclavian artery → PA.
Requires extensive dissection.
Risk of upper limb ischemia or subclavian steal phenomenon.
Modified BT: Graft connects SA → PA
Better growth of pulmonary tree and less distortion of PAs.
Long term patency.
A modified BT shunt does not cause arm ischemia or subclavian steal but can cause "coronary artery steal" owing to decreased coronary diastolic flow resulting from continuous forward flow through systemic into pulmonary circulation
Systemic-PA shunts are taken down during the subsequent Glenn procedure
Complications:
Seroma is an early complication (<30 days) of a modified BT shunt seen in 4%–20% of cases due to leakage through the graft.
Seroma is seen as a thin-walled loculated fluid collection surrounding the shunt.
Large seromas can cause lung compression and respiratory distress.
Shunt stenosis
Shunt thrombosis:
More common in men / preterm / high Hb / post surgical patent ductus
Central Shunts (Aorta - PA)
Shunt | Anastomosis |
Davidson | AscAorta → MPA using graft (PTFE) |
Mee | AscAorta → MPA (without graft) |
Waterston | Extrapericardial AscAo → RPA |
Cooley | Intrapericardial AscAo → RPA |
Potts | Posterior wall LPA → Anterior descending thoracic aorta |
SANO shunt | RV - PA conduit |
Central shunts have been abandoned due to complications:
Preferential blood flow to one lung → hypoplasia of the contralateral PA
Pulmonary overcirculation → Pulm Htn ++
Cardiac failure etc.
Modified central shunts have less PA distortion and symmetric flow to both PAs - but are more prone to thrombosis.
High-pressure pulsatile flow → can cause aneurysm / pseudoaneurysms.
Sano Shunt
RV - PA conduit
Non valved graft → free pulmonary regurgitation during diastole
First step in Norwood procedure.
Chosen over a central aortopulmonary shunt in a Norwood operation to prevent the diastolic "run-off" of blood from the aorta to the pulmonary circulation, thereby improving coronary artery perfusion.
Note: Not all RV-PA conduits called Sano Sano shunt is a specific palliative modification of the Stage 1 Norwood procedure, typically performed on neonates with Hypoplastic Left Heart Syndrome (HLHS) or other single-ventricle anomalies.
Why no valves in Sano?
In a neonate undergoing a Stage 1 Norwood procedure, the conduit is tiny—typically only 4-6 mm in diameter.
It is virtually impossible to engineer a functioning mechanical valve at that microscopic size.
Sluggish flow and the presence of valve leaflets would cause it to thrombose and occlude almost immediately.
The Hemodynamic Trade-Off: Sano vs. mBTT
Sano vs BT is a choice between pulmonary regurgitation (Sano) and coronary steal (mBTT).
The mBTT Problem (Diastolic Run-off): An mBTT connects the systemic arterial circulation (subclavian/innominate) to the low-pressure pulmonary system. Blood flows continuously from high to low pressure during both systole and diastole. This severely lowers the diastolic blood pressure in the aorta. Because the coronary arteries fill during diastole, this "diastolic run-off" steals blood away from the coronaries, placing the single right ventricle at a high risk for subendocardial ischemia or infarction.
The Sano Solution: By moving the shunt origin off the aorta and directly onto the right ventricle, the systemic arterial circulation is isolated. Diastolic blood pressure in the aorta remains high, ensuring excellent coronary perfusion.
Note: Biological RV-PA conduits (homografts and Contegra grafts) are highly prone to progressive, dense calcification over time. Sano shunts (PTFE) do not typically calcify but are prone to neointimal peeling and thrombosis.
Ductal Shunt
Also called "Wannabe BT shunt"
Useful in duct dependent Cyanotic diseases.
Potts Shunt
Posterior wall of LPA → Anterior aspect of ipsilateral descending thoracic aorta
Norwood Procedure
A palliative procedure that is the first of three stages in the surgical treatment of hypoplastic left heart syndrome.
The procedure consists of three components:
Constructing a neo-aorta by side-to-side anastomosis of the MPA and ascending aorta, such that the right ventricle supplies the systemic circulation
Creating a systemic-to-pulmonary shunt to provide some pulmonary blood flow
In the classic Norwood procedure, a modified Blalock-Taussig shunt is placed
In the Sano modification, a right ventricle-to-pulmonary artery conduit (Sano shunt) is used instead
Atrial septal resection
2. Systemic Venous → PA Shunts
Glenn
Fontan
Rastelli
Glenn Shunt [SVC → RPA]
Classic (Unidirectional) Glenn:
Proximal RPA is cut off from its origin.
Distal SVC transected.
End-to-end anastomosis of SVC - RPA.
Drawbacks:
Asymmetric growth of the pulmonary arteries, heavily favoring the right side while the left becomes hypoplastic.
Bidirectional Glenn:
Modern standard of care for Stage 2 single-ventricle palliation.
First is mBTT → → 2nd stage Glenn
MPA confluence is intact.
SVC is transected from the right atrium.
Anastomosed end-to-side to RPA.
Promotes symmetric growth of PAs.
Note:
Since this is a low-pressure - passive venous system, even mild anatomical narrowing can cause significant upstream congestion (SVC syndrome).
Assess the main confluence, RPA, and LPA for adequate, symmetric size Look for a patent azygous or hemiazygous vein, or other venovenous collaterals draining down into the IVC territory. Their presence suggests high pressures within the Glenn circuit (often due to elevated pulmonary vascular resistance or anatomical stenosis). Surgeons often ligate the azygous vein during a BD Glenn to prevent this "steal" of pulmonary blood flow.
Note the presence of antegrade flow through a native pulmonary valve or a residual patent aortopulmonary collateral (MAPCAs). Excessive accessory flow can increase pulmonary arterial pressure, hindering the passive venous drainage required for a successful Glenn circuit.
Fontan Procedure (Stage 3)
Performed between 2 to 4 years of age, this is the definitive palliation. By this age, the pulmonary vascular resistance has dropped sufficiently, and the pulmonary arteries have grown enough (promoted by the Stage 2 Glenn) to handle the entire systemic venous return passively.
The modern approach is the Total Cavopulmonary Connection (TCPC). While the Stage 2 Glenn routed the Superior Vena Cava (SVC) to the pulmonary arteries, the Fontan routes the Inferior Vena Cava (IVC) and hepatic venous return to the pulmonary arteries. This completely separates the red and blue blood.
Two main techniques are used:
Extracardiac Conduit: A synthetic Gore-Tex tube is sutured to the transected IVC, routed completely outside the heart, and anastomosed to the inferior aspect of the right pulmonary artery. This is currently the most favored approach as it avoids atrial incisions, reducing the risk of postoperative arrhythmias.
Lateral Tunnel (Intra-atrial Baffle): A synthetic patch is sewn inside the right atrium, creating a tunnel that baffles IVC blood up through the atrium and into the superior cavopulmonary connection.
The Fenestration: Surgeons often intentionally punch a 4–5 mm hole (fenestration) in the Fontan conduit or baffle, allowing a small amount of deoxygenated blood to escape into the functional single atrium. This acts as a crucial "pop-off valve." While it causes mild cyanosis, it preserves cardiac output if pulmonary pressures acutely rise in the postoperative period.
Imaging Objectives (Post-Stage 3):
Pathway Patency: Evaluate the entire TCPC pathway (IVC → Conduit/Baffle → PAs) for sluggish flow, spontaneous echo contrast (smoke), or frank thrombosis, as this is a low-pressure, passive venous system highly prone to clot formation.
Fenestration Evaluation: Determine if a surgically created fenestration is patent or has spontaneously closed.
Fontan-Associated Liver Disease (FALD): The chronically elevated central venous pressure required to drive blood passively through the pulmonary bed leads to hepatic congestion, fibrosis, and eventual cirrhosis. Cross-sectional imaging of the liver is a mandatory component of long-term Fontan surveillance.
Collaterals: Evaluate for venovenous collaterals (which bypass the lungs and worsen cyanosis) or aortopulmonary collaterals (which increase the volume load on the single ventricle).



Comments